Background: Neoadjuvant chemotherapy followed by surgery and subsequent adjuvant chemotherapy has been a mainstay of many osteosarcoma treatment protocols. However, the overall survival (OS) benefit over surgery and adjuvant chemotherapy is unclear. Aims: This study therefore directly compares the outcomes among these treatment groups using a large population in the National Cancer Database (NCDB). Methods: In a retrospective cross-sectional study, osteosarcoma patients in the NCDB (2004-2019) were stratified based on chemotherapy and surgery timing (neoadjuvant and adjuvant vs adjuvant-only chemotherapy). We used Kaplan-Meier curves to compare OS in the unmatched population and in a propensity score matched cohort that controlled for demographics, treatment, and tumor characteristic differences. Univariate and multivariate analyses were also used to predict the likelihood of positive margins among the population. Chi-square tests were used to compare 30- and 90-day mortality among treatment groups. P-values <0.05 were considered significant. Results: The study population included 4,659 patients: 3,733 neoadjuvant and 926 adjuvant-only chemotherapy regimens. Patients who underwent neoadjuvant therapy had significantly longer survival in the unmatched analysis (p<0.001), but this difference narrowed when controlling for covariates in the matched cohort (p=0.67). Mortality at 30 and 90 days was insignificant between treatment groups in both the full and matched cohorts (p=0.3 and p=0.9 respectively). Neoadjuvant chemotherapy regimens predominated with over 75% utilization, but this rate remained constant during the 15-year study period. Three- and five-year survival rates were relatively unchanged during this period at 75% and 62.5% respectively. Factors significantly associated with positive margins in the multivariate analysis included adjuvant-only chemotherapy (OR=1.6, p<0.001), older age (OR=1.01, p<0.001), female sex (OR=1.27, p=0.04), adjuvant radiation (OR=4.96, p<0.001), and stage IVB tumors (OR=2.11, p<0.001). Conclusions: These results indicate that neoadjuvant chemotherapy did not increase overall or short-term survival compared to adjuvant chemotherapy alone in our study. However, neoadjuvant therapy was associated with fewer positive margins at the time of surgery. These insights offer information to help clinicians evaluate osteosarcoma treatment regimens to maximize outcomes and limit treatment morbidity.
| Published in | Journal of Cancer Treatment and Research (Volume 13, Issue 1) |
| DOI | 10.11648/j.jctr.20251301.12 |
| Page(s) | 10-22 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Osteosarcoma, Chemotherapy, Survival Analysis, Margins of Excision, Morbidity, National Cancer Database (NCDB)
Characteristics | Neoadjuvant | Adjuvant | P-value |
|---|---|---|---|
N = 3,733 | N = 926 | ||
Age | 17 [13, 28] | 34 [20, 52] | <.001 |
Sex | .027 | ||
Male | 2,208 (59.1) | 510 (55.1) | |
Female | 1,525 (40.9) | 416 (44.9) | |
Race | .3 | ||
White | 2,764 (74.0) | 698 (75.4) | |
Black | 588 (15.8) | 153 (16.5) | |
Asian American and Pacific Islander (AAPI) | 198 (5.3) | 37 (4.0) | |
Unknown | 183 (4.9) | 38 (4.1) | |
Ethnicity | <.001 | ||
Non-Hispanic | 3,039 (81.4) | 772 (83.4) | |
Hispanic | 587 (15.7) | 109 (11.8) | |
Unknown | 107 (2.9) | 45 (4.9) | |
Charlson-Deyo Comorbidity Index | .082 | ||
0 | 3,451 (92.4) | 838 (90.5) | |
1 | 243 (6.5) | 72 (7.8) | |
2+ | 39 (1.0) | 16 (4.9) | |
Insurance Status | <.001 | ||
Private | 2,328 (62.4) | 548 (59.2) | |
Medicare | 130 (3.5) | 108 (11.7) | |
Medicaid | 937 (25.1) | 182 (19.7) | |
Other Government | 86 (2.3) | 14 (1.5) | |
Uninsured | 141 (3.8) | 46 (5.0) | |
Unknown | 111 (3.0) | 28 (3.0) | |
Facility Type | .018 | ||
Non-Academic | 836 (22.4) | 230 (24.8) | |
Academic | 2,682 (71.8) | 662 (71.5) | |
Unknown | 215 (5.8) | 34 (3.7) | |
Radiation | <.001 | ||
No Radiation | 3,501 (93.8) | 782 (84.4) | |
Neoadjuvant | 29 (0.8) | 10 (1.1) | |
Adjuvant | 96 (2.6) | 96 (10.4) | |
Unknown | 107 (2.9) | 38 (4.1) | |
Surgery | <.001 | ||
Local Excision or Destruction | 151 (4.0) | 109 (11.8) | |
Partial Resection | 209 (5.6) | 102 (11.0) | |
Radical Excision and Limb Salvage | 2,612 (70.0) | 525 (56.7) | |
Amputation | 761 (20.4) | 190 (20.5) | |
Margins | <.001 | ||
Positive | 239 (6.4) | 120 (13.0) | |
Negative | 3,250 (87.1) | 689 (74.4) | |
Unknown | 244 (6.5) | 117 (12.6) | |
Clinical TNM Staging | |||
7th Edition (’04-’17) | <.001 | ||
IA | 310 (9.8) | 111 (13.5) | |
IB | 293 (9.3) | 56 (6.8) | |
IIA | 728 (23.0) | 244 (29.7) | |
IIB | 1,229 (38.9) | 261 (31.8) | |
III | 83 (2.6) | 26 (3.2) | |
IVA | 346 (11.0) | 346 (11.0) | |
IVB | 170 (5.4) | 170 (5.4) | |
8th Edition (’18-’19) | .07 | ||
IA | 67 (11.7) | 21 (20.0) | |
IB | 61 (10.6) | 15 (14.3) | |
IIA | 142 (24.7) | 26 (24.8) | |
IIB | 173 (30.1) | 21 (20.0) | |
III | 21 (3.7) | 3 (2.9) | |
IVA | 83 (14.5) | 11 (10.5) | |
IVB | 27 (4.7) | 8 (7.6) | |
Tumor Location | <.001 | ||
Head | 174 (4.7) | 162 (17.5) | |
Axial | 240 (6.4) | 136 (14.7) | |
Appendicular | 3,290 (88.1) | 611 (66.0) | |
Unknown | 29 (0.8) | 17 (1.8) |
Characteristics | Neoadjuvant | Adjuvant | SMD |
|---|---|---|---|
N = 872 | N = 872 | ||
Age | 31 [17, 51] | 31 [19, 48] | 0.019 |
Year of Diagnosis | 2011 [2007, 2014] | 2011 [2007, 2015] | 0.038 |
Sex | 0.007 | ||
Male | 488 (55.5) | 485 (55.2) | |
Female | 388 (44.5) | 391 (44.8) | |
Race | 0.059 | ||
White | 637 (73.1) | 655 (75.1) | |
Black | 162 (18.6) | 146 (16.7) | |
AAPI | 32 (3.7) | 35 (4.0) | |
Unknown | 41 (4.7) | 36 (4.1) | |
Ethnicity | 0.025 | ||
Non-Hispanic | 728 (83.5) | 722 (82.8) | |
Hispanic | 101 (11.6) | 108 (12.4) | |
Unknown | 43 (4.9) | 42 (4.8) | |
Charlson-Deyo Comorbidity Index | 0.018 | ||
0 | 789 (90.5) | 787 (90.3) | |
1 | 69 (7.69) | 69 (7.9) | |
2+ | 14 (1.6) | 16 (1.8) | |
Insurance Status | 0.084 | ||
Private | 511 (58.6) | 518 (59.4) | |
Medicare | 77 (8.8) | 91 (10.4) | |
Medicaid | 181 (20.8) | 177 (20.3) | |
Other Government | 19 (2.2) | 14 (1.6) | |
Uninsured | 50 (5.7) | 45 (5.2) | |
Unknown | 34 (3.9) | 27 (3.1) | |
Facility Type | 0.005 | ||
Non-Academic | 211 (24.2) | 209 (24.0) | |
Academic | 628 (72.0) | 630 (72.2) | |
Unknown | 33 (3.8) | 33 (3.8) | |
Radiation | 0.052 | ||
No Radiation | 762 (87.4) | 755 (86.6) | |
Neoadjuvant | 13 (1.5) | 10 (1.1) | |
Adjuvant | 63 (7.2) | 73 (8.4) | |
Unknown | 34 (3.9) | 34 (3.9) | |
Surgery | 0.099 | ||
Local Excision or Destruction | 77 (8.8) | 88 (10.1) | |
Partial Resection | 80 (9.2) | 91 (10.4) | |
Radical Excision and Limb Salvage | 496 (56.9) | 507 (58.1) | |
Amputation | 219 (25.1) | 186 (21.3) | |
Margins | 0.055 | ||
Positive | 108 (12.4) | 105 (12.0) | |
Negative | 677 (77.6) | 665 (76.3) | |
Unknown | 87 (10.0) | 102 (11.7) | |
Clinical TNM Staging | 0.082 | ||
7th Edition (’04-’17) | |||
IA | 100 (11.5) | 96 (11.0) | |
IB | 65 (7.5) | 54 (6.2) | |
IIA | 218 (25.0) | 229 (26.3) | |
IIB | 258 (29.6) | 250 (28.7) | |
III | 21 (2.4) | 22 (2.5) | |
IVA | 62 (7.1) | 67 (7.7) | |
IVB | 48 (5.5) | 52 (6.0) | |
8th Edition (’18-’19) | |||
IA | 17 (1.9) | 19 (2.2) | |
IB | 16 (1.8) | 15 (1.7) | |
IIA | 25 (2.9) | 26 (3.0) | |
IIB | 17 (1.9) | 21 (2.4) | |
III | 4 (0.5) | 3 (0.3) | |
IVA | 14 (1.6) | 11 (1.3) | |
IVB | 7 (0.8) | 7 (0.8) | |
Tumor Location | 0.028 | ||
Head | 129 (14.8) | 137 (15.7) | |
Axial | 117 (13.4) | 118 (13.5) | |
Appendicular | 612 (70.2) | 604 (69.3) | |
Unknown | 14 (1.6) | 13 (1.5) |
Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
OR | P value | OR | P value | |
Age | 1.02 | <0.001 | 1.01 | <0.001 |
Sex | ||||
Male | (Ref) | --- | ||
Female | 1.28 | 0.02 | 1.27 | 0.04 |
Race | ||||
White | (Ref) | --- | ||
Black | 1.15 | 0.3 | ||
Asian and Pacific Islander | 0.41 | 0.01 | 0.37 | 0.008 |
Ethnicity | ||||
Non-Hispanic | (Ref) | --- | ||
Hispanic | 0.80 | 0.2 | ||
Charleson-Deyo Score | ||||
0 | (Ref) | --- | ||
1 | 0.88 | 0.6 | ||
2+ | 2.21 | 0.03 | 1.69 | 0.2 |
Insurance Status | ||||
Private | (Ref) | --- | ||
Medicare | 1.97 | 0.001 | 0.94 | 0.1 |
Medicaid | 0.93 | 0.6 | ||
Other Government | 1.74 | 0.07 | 1.70 | 0.8 |
Uninsured | 1.02 | 0.9 | ||
Facility Type | ||||
Non-Academic | (Ref) | --- | ||
Academic | 0.74 | 0.02 | 0.75 | 0.02 |
Radiation | ||||
No Radiation | (Ref) | --- | ||
Neoadjuvant | 1.72 | 0.3 | ||
Adjuvant | 7.55 | <0.001 | 4.96 | <0.001 |
Chemotherapy | ||||
Neoadjuvant | (Ref) | --- | ||
Adjuvant | 2.37 | <0.001 | 1.60 | <0.001 |
Stage | ||||
IA | (Ref) | --- | ||
IB | 0.77 | 0.3 | ||
IIA | 0.96 | 0.8 | ||
IIB | 0.67 | 0.03 | 0.81 | 0.1 |
III | 0.69 | 0.4 | ||
IVA | 1.04 | 0.9 | ||
IVB | 2.24 | <0.001 | 2.11 | <0.001 |
Year of Diagnosis | 0.99 | 0.7 | ||
OS | Overall Survival |
NCDB | National Cancer Database |
DFS | Disease-free Survival |
CoC | Commission on Cancer |
NA | Neoadjuvant |
AO | Adjuvant-only |
AAPI | Asian American and Pacific Islander |
OR | Odds Ratio |
SMD | Standardized Mean Difference |
MAP | Methotrexate, Doxorubicin, and Cisplatin |
| [1] | Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. Cancer Treat Res 2009; 152: 3–13. |
| [2] |
SEER Stat Fact Sheets: Bone and Joint Cancer n.d.
https://seer.cancer.gov/statfacts/html/bones.html (accessed December 28, 2023). |
| [3] | Linabery AM, Ross JA. Trends in childhood cancer incidence in the U.S. (1992-2004). Cancer 2008; 112: 416–32. |
| [4] | Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004. Cancer 2009; 115: 1531–43. |
| [5] | Choi JH, Ro JY. The 2020 WHO Classification of Tumors of Bone: An Updated Review. Adv Anat Pathol 2021; 28: 119–38. |
| [6] | Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. International classification of childhood cancer, third edition. Cancer 2005; 103: 1457–67. |
| [7] | Ritter J, Bielack SS. Osteosarcoma. Ann Oncol 2010; 21 Suppl 7. |
| [8] | Luetke A, Meyers PA, Lewis I, Juergens H. Osteosarcoma treatment - where do we stand? A state of the art review. Cancer Treat Rev 2014; 40: 523–32. |
| [9] | Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002; 20: 776–90. |
| [10] |
Pathology and Genetics of Tumours of Soft Tissue and Bone - World Health Organization - Google Books n.d.
https://books.google.com/books?hl=en&lr=&id=dg9am0g4EP8C&oi=fnd&pg=PA3&ots=zwpcTNfqn4&sig=UhEaNk0hVCvbzuwUURW1xsnSct8#v=onepage&q&f=false (accessed December 28, 2023). |
| [11] | Daw NC, Chou AJ, Jaffe N, Rao BN, Billups CA, Rodriguez-Galindo C, et al. Recurrent osteosarcoma with a single pulmonary metastasis: A multi-institutional review. Br J Cancer 2015; 112: 278–82. |
| [12] | Mettmann VL, Baumhoer D, Bielack SS, Blattmann C, Friedel G, von Kalle T, et al. Solitary pulmonary metastases at first recurrence of osteosarcoma: Presentation, treatment, and survival of 219 patients of the Cooperative Osteosarcoma Study Group. Cancer Med 2023; 12: 18219–34. |
| [13] | Arndt CAS, Crist WM. Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999; 341: 342–52. |
| [14] | Bielack S, Jürgens H, Jundt G, Kevric M, Kühne T, Reichardt P, et al. Osteosarcoma: the COSS experience. Cancer Treat Res 2009; 152: 289–308. |
| [15] | Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res 2006; 450: 164–71. |
| [16] | Kudawara I, Aoki Y, Ueda T, Araki N, Naka N, Nakanishi H, et al. Neoadjuvant and adjuvant chemotherapy with high-dose ifosfamide, doxorubicin, cisplatin and high-dose methotrexate in non-metastatic osteosarcoma of the extremities: A phase II trial in Japan. Journal of Chemotherapy 2013; 25: 41–8. |
| [17] | Yamamoto N, Tsuchiya H. Chemotherapy for osteosarcoma - Where does it come from? What is it? Where is it going? Expert Opin Pharmacother 2013; 14: 2183–93. |
| [18] |
Delepine N, Delepine G, Bacci G, Rosen G, Desbois JC. Influence of methotrexate dose intensity on outcome of patients with high grade osteogenic osteosarcoma: Analysis of the literature. Cancer 1996; 78: 2127–35.
https://doi.org/10.1002/(SICI)1097-0142(19961115)78:10<2127::AID-CNCR13>3.0.CO;2-0 |
| [19] | Casali PG, Bielack S, Abecassis N, Aro HT, Bauer S, Biagini R, et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2018; 29: iv79–95. |
| [20] | Ismail M, Wiratnaya IG, Raditya R. Evaluating the Outcome and Patient Safety of Methotrexate, Doxorubicin, and Cisplatin Regimen for Chemotherapy in Osteosarcoma: A Meta-Analysis. Asian Pacific Journal of Cancer Prevention 2024; 25: 1497–505. |
| [21] | Adewuyi E, Chorya H, Muili A, Moradeyo A, Kayode A, Naik A, et al. Chemotherapy, immunotherapy, and targeted therapy for osteosarcoma: Recent advancements. Crit Rev Oncol Hematol 2025; 206: 104575. |
| [22] | Goorin AM, Schwartzentruber DJ, Devidas M, Gebhardt MC, Ayala AG, Harris MB, et al. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J Clin Oncol 2003; 21: 1574–80. |
| [23] | Provisor AJ, Ettinger LJ, Nachman JB, Krailo MD, Makley JT, Yunis EJ, et al. Treatment of nonmetastatic osteosarcoma of the extremity with preoperative and postoperative chemotherapy: a report from the Children’s Cancer Group. J Clin Oncol 1997; 15: 76–84. |
| [24] | Soares do Brito J, Santos R, Sarmento M, Fernandes P, Portela J. Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes. Curr Oncol 2023; 30: 6148–65. |
| [25] | Foroughi A, Arefpour AM, Nikoofar A, Sanei M, Mahdavi SH, Javadinia SA. Total Neoadjuvant vs. Standard Perioperative Cisplatin/ Doxorubicin Chemotherapy in Patients with Extremities Osteosarcoma: A Multi-Center Cohort Study. Asian Pacific Journal of Cancer Prevention 2023; 24: 2369–74. |
| [26] | Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al. Chemotherapy for nonmetastatic osteogenic sarcoma: the Memorial Sloan-Kettering experience. J Clin Oncol 1992; 10: 5–15. |
| [27] | Austin PC. The performance of different propensity score methods for estimating marginal hazard ratios. Stat Med 2013; 32: 2837–49. |
| [28] |
Rosen G, Suwansirikul S, Kwon C, Tan C, Wu SJ, Beattie EJ, et al. High-dose methotrexate with citrovorum factor rescue and adriamycin in childhood osteogenic sarcoma. Cancer 1974; 33: 1151–63.
https://doi.org/10.1002/1097-0142(197404)33:4<1151::AID-CNCR2820330439>3.0.CO;2-8 |
| [29] | Eilber F, Giuliano A, Eckardt J, Patterson K, Moseley S, Goodnight J. Adjuvant chemotherapy for osteosarcoma: a randomized prospective trial. Journal of Clinical Oncology 1987; 5: 21–6. |
| [30] | Link MP, Goorin AM, Miser AW, Green AA, Pratt CB, Belasco JB, et al. The Effect of Adjuvant Chemotherapy on Relapse-Free Survival in Patients with Osteosarcoma of the Extremity. New England Journal of Medicine 1986; 314: 1600–6. |
| [31] | Bielack S, Carrle D, Casali PG. Osteosarcoma: ESMO Clinical Recommendations for diagnosis, treatment and follow-up. Annals of Oncology 2009; 20: iv137–9. |
| [32] |
Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG. Primary osteogenic sarcoma. The rationale for preoperative chemotherapy and delayed surgery. Cancer 1979; 43: 2163–77.
https://doi.org/10.1002/1097-0142(197906)43:6<2163::AID-CNCR2820430602>3.0.CO;2-S. |
| [33] |
Rosen G, Caparros B, Huvos AG, Kosloff C, Nirenberg A, Cacavio A, et al. Preoperative chemotherapy for osteogenic sarcoma: Selection of postoperative adjuvant chemotherapy based on the response of the primary tumor to preoperative chemotherapy. Cancer 1982; 49: 1221–30.
https://doi.org/10.1002/1097-0142(19820315)49:6<1221::AID-CNCR2820490625>3.0.CO;2-E |
| [34] | Avella M, Bacci G, McDonald DJ, Di Scioscio M, Picci P, Campanacci M. Adjuvant chemotherapy with six drugs (adriamycin, methotrexate, cisplatinum, bleomycin, cyclophosphamide and dactinomycin) for non-metastatic high grade osteosarcoma of the extremities. Results of 32 patients and comparison to 127 patients concomitantly treated with the same drugs in a neoadjuvant form. Chemioterapia 1988; 7: 133–7. |
| [35] | Marina NM, Smeland S, Bielack SS, Bernstein M, Jovic G, Krailo MD, et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): an open-label, international, randomised controlled trial. Lancet Oncol 2016; 17: 1396–408. |
| [36] | Bielack SS, Machatschek JN, Flege S, Jürgens H. Delaying surgery with chemotherapy for osteosarcoma of the extremities. Expert Opin Pharmacother 2004; 5: 1243–56. |
| [37] | Shim T, Chillakuru Y, Darwish C, Chalif E, Strum D, Benito DA, et al. Head and neck osteosarcomas: Analysis of treatment trends and survival outcomes in the United States (2004-2016). Head Neck 2021; 43: 3294–305. |
| [38] | Hosalkar HS, Dormans JP. Limb sparing surgery for pediatric musculoskeletal tumors. Pediatr Blood Cancer 2004; 42: 295–310. |
| [39] | Smeland S, Bielack SS, Whelan J, Bernstein M, Hogendoorn P, Krailo MD, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur J Cancer 2019; 109: 36–50. |
APA Style
Dotson, L. J., Blackburn, K. W., Mand, D., Trudeau, T., Agarwal, R., et al. (2025). Comparing the Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy for Osteosarcoma Patients. Journal of Cancer Treatment and Research, 13(1), 10-22. https://doi.org/10.11648/j.jctr.20251301.12
ACS Style
Dotson, L. J.; Blackburn, K. W.; Mand, D.; Trudeau, T.; Agarwal, R., et al. Comparing the Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy for Osteosarcoma Patients. J. Cancer Treat. Res. 2025, 13(1), 10-22. doi: 10.11648/j.jctr.20251301.12
AMA Style
Dotson LJ, Blackburn KW, Mand D, Trudeau T, Agarwal R, et al. Comparing the Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy for Osteosarcoma Patients. J Cancer Treat Res. 2025;13(1):10-22. doi: 10.11648/j.jctr.20251301.12
@article{10.11648/j.jctr.20251301.12,
author = {Luke James Dotson and Kyle Warren Blackburn and Davinder Mand and Trevor Trudeau and Rashmi Agarwal and Russell Alan Ward},
title = {Comparing the Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy for Osteosarcoma Patients
},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {1},
pages = {10-22},
doi = {10.11648/j.jctr.20251301.12},
url = {https://doi.org/10.11648/j.jctr.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251301.12},
abstract = {Background: Neoadjuvant chemotherapy followed by surgery and subsequent adjuvant chemotherapy has been a mainstay of many osteosarcoma treatment protocols. However, the overall survival (OS) benefit over surgery and adjuvant chemotherapy is unclear. Aims: This study therefore directly compares the outcomes among these treatment groups using a large population in the National Cancer Database (NCDB). Methods: In a retrospective cross-sectional study, osteosarcoma patients in the NCDB (2004-2019) were stratified based on chemotherapy and surgery timing (neoadjuvant and adjuvant vs adjuvant-only chemotherapy). We used Kaplan-Meier curves to compare OS in the unmatched population and in a propensity score matched cohort that controlled for demographics, treatment, and tumor characteristic differences. Univariate and multivariate analyses were also used to predict the likelihood of positive margins among the population. Chi-square tests were used to compare 30- and 90-day mortality among treatment groups. P-values Results: The study population included 4,659 patients: 3,733 neoadjuvant and 926 adjuvant-only chemotherapy regimens. Patients who underwent neoadjuvant therapy had significantly longer survival in the unmatched analysis (pConclusions: These results indicate that neoadjuvant chemotherapy did not increase overall or short-term survival compared to adjuvant chemotherapy alone in our study. However, neoadjuvant therapy was associated with fewer positive margins at the time of surgery. These insights offer information to help clinicians evaluate osteosarcoma treatment regimens to maximize outcomes and limit treatment morbidity.
},
year = {2025}
}
TY - JOUR T1 - Comparing the Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy for Osteosarcoma Patients AU - Luke James Dotson AU - Kyle Warren Blackburn AU - Davinder Mand AU - Trevor Trudeau AU - Rashmi Agarwal AU - Russell Alan Ward Y1 - 2025/05/29 PY - 2025 N1 - https://doi.org/10.11648/j.jctr.20251301.12 DO - 10.11648/j.jctr.20251301.12 T2 - Journal of Cancer Treatment and Research JF - Journal of Cancer Treatment and Research JO - Journal of Cancer Treatment and Research SP - 10 EP - 22 PB - Science Publishing Group SN - 2376-7790 UR - https://doi.org/10.11648/j.jctr.20251301.12 AB - Background: Neoadjuvant chemotherapy followed by surgery and subsequent adjuvant chemotherapy has been a mainstay of many osteosarcoma treatment protocols. However, the overall survival (OS) benefit over surgery and adjuvant chemotherapy is unclear. Aims: This study therefore directly compares the outcomes among these treatment groups using a large population in the National Cancer Database (NCDB). Methods: In a retrospective cross-sectional study, osteosarcoma patients in the NCDB (2004-2019) were stratified based on chemotherapy and surgery timing (neoadjuvant and adjuvant vs adjuvant-only chemotherapy). We used Kaplan-Meier curves to compare OS in the unmatched population and in a propensity score matched cohort that controlled for demographics, treatment, and tumor characteristic differences. Univariate and multivariate analyses were also used to predict the likelihood of positive margins among the population. Chi-square tests were used to compare 30- and 90-day mortality among treatment groups. P-values Results: The study population included 4,659 patients: 3,733 neoadjuvant and 926 adjuvant-only chemotherapy regimens. Patients who underwent neoadjuvant therapy had significantly longer survival in the unmatched analysis (pConclusions: These results indicate that neoadjuvant chemotherapy did not increase overall or short-term survival compared to adjuvant chemotherapy alone in our study. However, neoadjuvant therapy was associated with fewer positive margins at the time of surgery. These insights offer information to help clinicians evaluate osteosarcoma treatment regimens to maximize outcomes and limit treatment morbidity. VL - 13 IS - 1 ER -
School of Medicine, Baylor College of Medicine; Houston, USA
School of Medicine, Baylor College of Medicine; Houston, USA
Department of Orthopedic Surgery, Baylor Scott & White Health, Temple, USA
School of Medicine, Baylor College of Medicine; Houston, USA
Department of Orthopedic Surgery, Baylor Scott & White Health, Temple, USA
Department of Orthopedic Surgery, Baylor Scott & White Health, Temple, USA
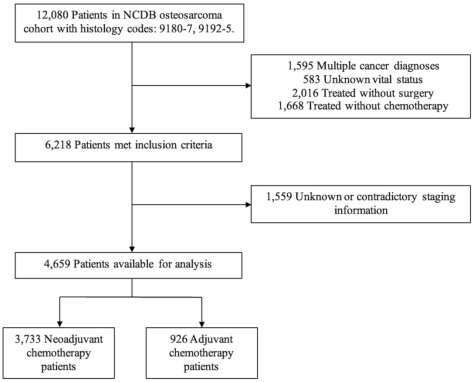
Figure 1. STROBE based diagram showing patient selection for this study.
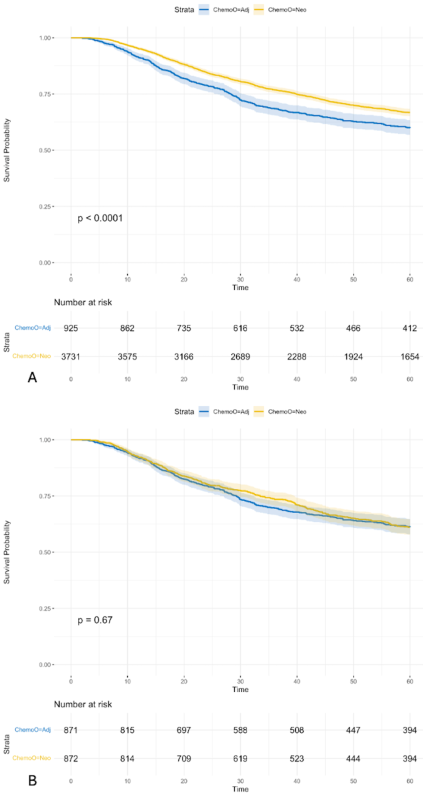
Figure 2. The unmatched (A) and propensity score matched (B) survival comparisons based on chemotherapy timing. Time is measured in months.
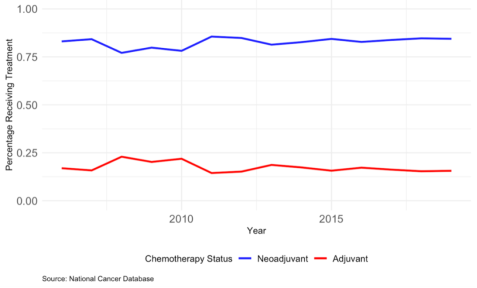
Figure 3. The above figure shows the trends in treatment over time (annual basis) for neoadjuvant vs adjuvant chemotherapy.
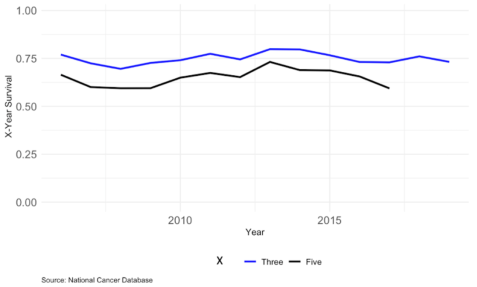
Figure 4. The above figure shows the trends in 3- and 5-year survival over the study period.
Information

